
The Care Plan offers a written framework to document the outcome of the care planning process. This may involve client and staff-defined goals, assessment and/or treatment information, Referrals, Encounters, and Procedures requested throughout the care planning process. The Care Plan has a history form which makes previous plan information readily accessible. The Care Plan has tabs for each of these actions. An image of each is captured below.
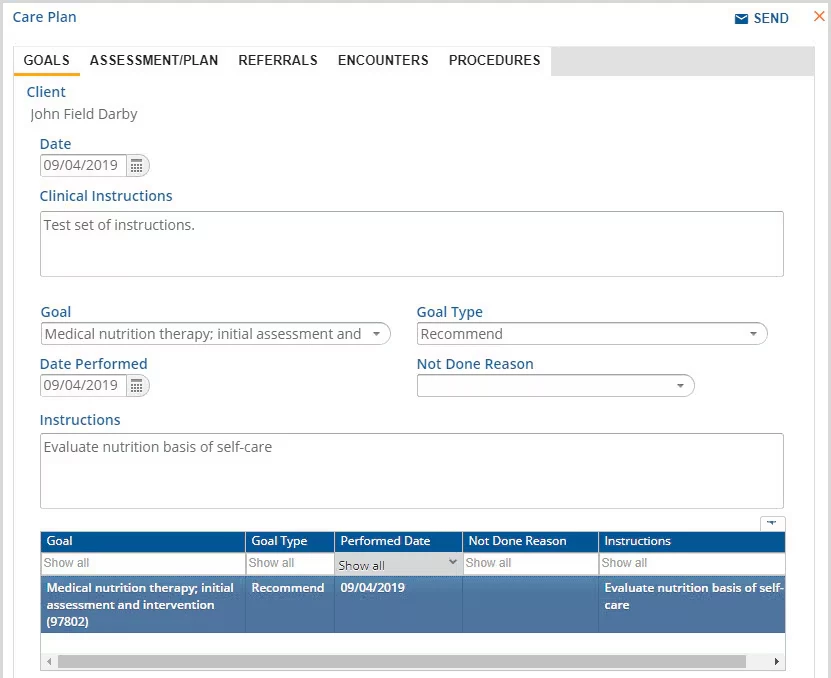
Goals
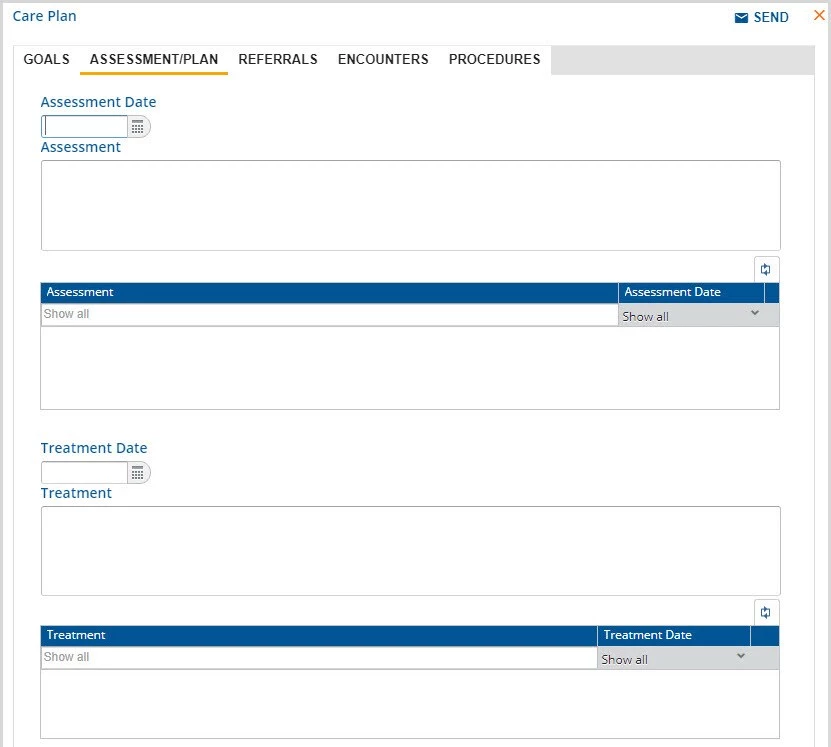
Assessment/Plan
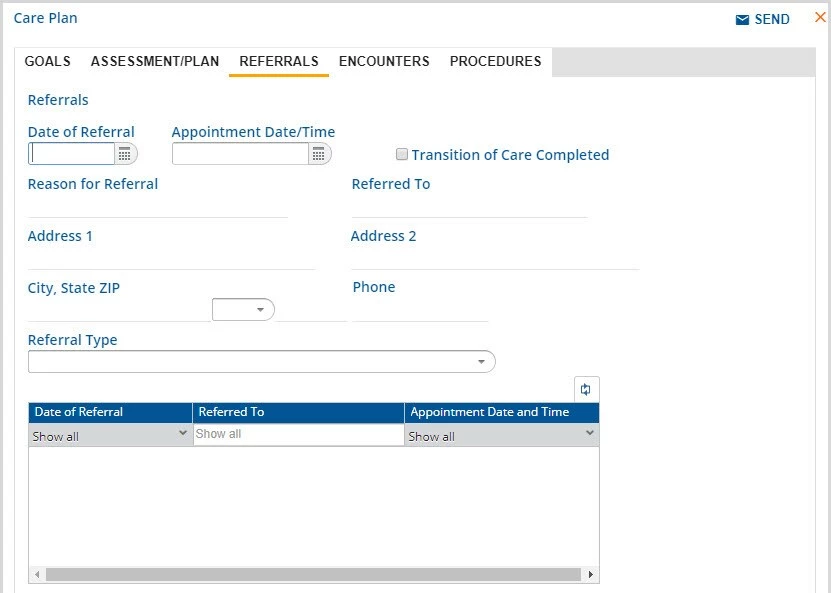
Referrals
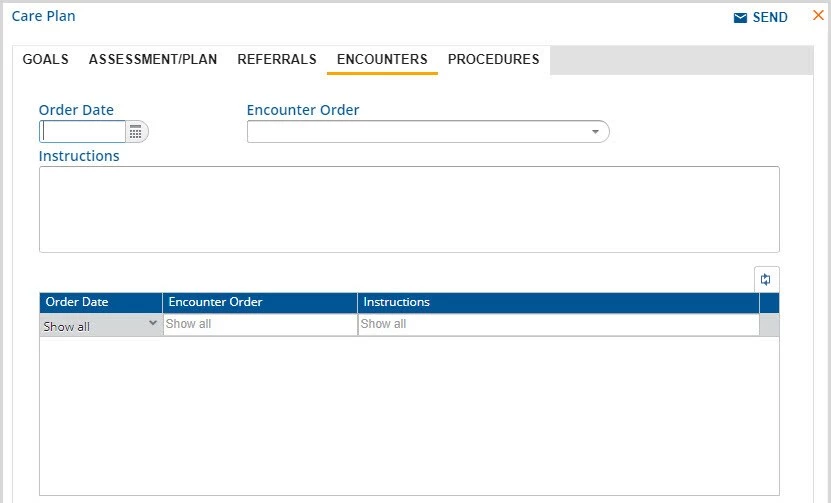
Encounters
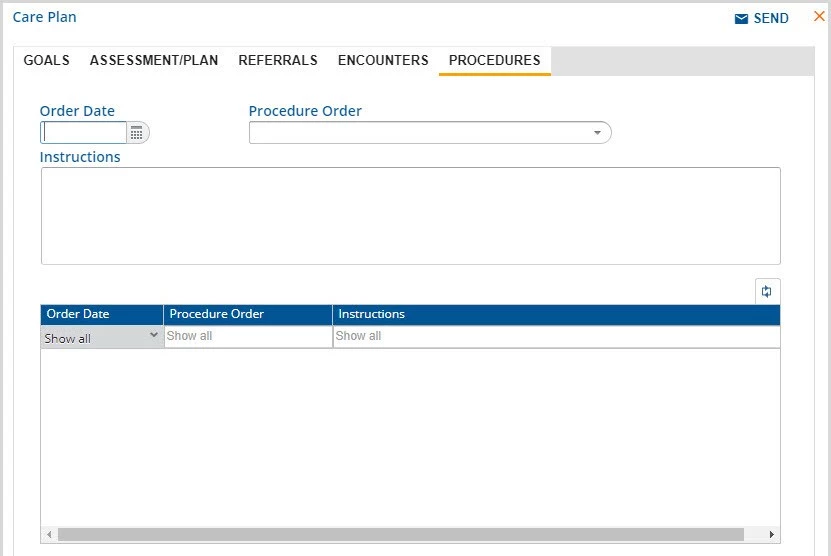
Procedures